Private Ultrasound Scans are an essential part of infertility testing and fertility treatment. If you have had a child before, you may be familiar with the kind of ultrasound done during mid to late pregnancy. Even if you have never had a child, you may have seen pregnancy ultrasound exams on movies or television. Or, perhaps, a friend or family member may have shared an ultrasound image of their unborn child with you.
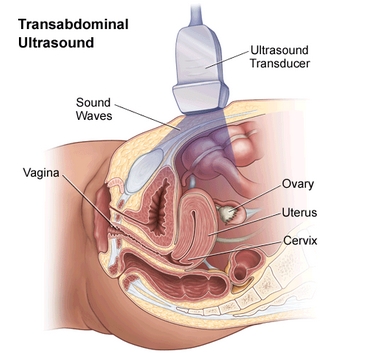
Ultrasounds done during mid to late pregnancy are usually abdominal ultrasounds. In other words, a transducer (a device that emits and receives sound waves for an ultrasound) is moved around over the abdomen.
For fertility testing and treatment, the majority of ultrasounds are done transvaginally; that is to say via the vagina with a slender specialized wand.
Ultrasounds scan are not painful, though they can be slightly uncomfortable.
During infertility testing, ultrasound scans can provide information on the ovaries, endometrial lining, and uterus. Specialized ultrasounds can be used to evaluate ovarian reserves, the uterine shape in more detail, and whether the fallopian tubes are open or blocked.
During fertility treatment, ultrasound is used to monitor follicle development in the ovaries and the thickness of the endometrial lining. Ultrasound is also used during IVF for egg retrieval, to guide the needle through the vaginal wall to the ovaries. Some doctors use ultrasound during embryo transfer.
If you get pregnant, your reproductive endocrinologist will likely order a few ultrasounds before transferring you back to your regular OB/GYN.
Infertility Ultrasound Scan Basics
Ultrasound scans work by using high-frequency sound waves to create an image of your internal organs. You won’t be able to hear the sound waves.
A transducer is a device used during an ultrasound to emit and receive these high-frequency sound waves. During fertility testing and treatment, the technician is likely to use two different kinds of transducer devices; one that is used for abdominal ultrasound and a second that is used transvaginally.
During an abdominal ultrasound, a gel is squirted over your abdomen. Then, the transducer is gently moved over the abdomen. The gel makes it easier for the transducer to slide around over your skin.
During a transvaginal ultrasound, the transducer is shaped like a slender, long wand. A condom is placed over the wand and a lubricant gel is generously squirted over the condom.
The technician will hand you the handle of the transducer wand, so you can place the transducer gently inside of your vagina as far as it will comfortably go. You will then hand off the handle to the technician, who will conduct the exam.
Sound waves are emitted by the transducer. They echo (or bounce back) when they hit your internal organs. The ultrasound machine interprets these signals and turns them into a digital image.
Before an abdominal ultrasound, your doctor will likely ask you to drink several cups of water in the hours before your exam but request that you don’t relieve yourself if you feel the need to urinate. (You probably will feel the urge to go!)
A full bladder pushes your intestines out of the way, so your reproductive organs are easier to see. Once the abdominal ultrasound is finished, you will be able to use the bathroom.
However, to see the detail needed for fertility testing and treatment, transvaginal ultrasound provides even better imagery.
The transvaginal transducer tip is placed right below the cervix, which is closer to your reproductive organs.
Beside the abdominal and transvaginal ultrasound, there are other specialized ultrasound scans that your doctor may request.
Antral follicle count ultrasound: this is done with the usual transvaginal ultrasound device, but requires special training for the technician to complete accurately. Antral follicle count ultrasounds can help determine your ovarian reserves and possibly help diagnose polycystic ovarian syndrome (PCOS). You may or may not have an antral follicle count exam as part of your basic fertility workup.
This may also be scheduled separately or at the same time as a general ultrasound scan.
3D ultrasound: Most ultrasound imagery is two-dimensional. Advancing technology now can also generate three-dimensional images. This allows for better detection of some uterine abnormalities and fallopian tube problems that are not visible on a typical 2D ultrasound scan.
Sonohysterogram: A sonohysterogram is a specialized ultrasound that involves transferring a saline solution into the uterus via a catheter. The saline solution fills your uterus, making it easier to visualize the shape and any possible adhesions within. A sonohysterogram may be done during a basic fertility workup, but is more commonly used for specific situations.
Hysterosalpingo-contrast sonography (HyCoSy): This is similar to a sonohysterography, except a dye or a saline solution mixed with air bubbles is used to determine whether the fallopian tubes are open or blocked. It’s more common for doctors to evaluate whether the fallopian tubes are open with an HSG, which is a specialized X-ray. The advantages of having an HyCoSy over an HSG are that the HyCoSy may cause less discomfort than an HSG. HyCoSy doesn’t require radiation or iodine exposure. An HyCoSy may be done at the same time as a general ultrasound exam (which would mean one less appointment).
What Your Doctor Is Evaluating With Ultrasound
Here is what your fertility doctor is evaluating with an infertility ultrasound scan.
General position and presence of the reproductive organs: Is everything that should be there present? Is everything in the correct area?
It seems like a very basic question, but some women are born without the ovaries or their uterus.
The ovaries: The ultrasound tech will look at your ovaries. She will take note of their size and shape.
She will also look for evidence of both normal and not normal cysts on the ovaries. Many small cysts that look like a pearl necklace may indicate polycystic ovarian syndrome. The presence of a larger endometrioma cyst may indicate possible endometriosis.
In rare cases, a mass that is not a cyst may be found on the ovaries.
Antral follicle count: This may be part of a general infertility ultrasound scan or may be scheduled separately. Antral follicles are a specific kind of follicle found in the ovaries. They are part of the egg/oocyte lifecycle.
A very low antral follicle count may indicate poor ovarian reserves. An unusually high antral follicle count may indicate PCOS.
The uterus: The ultrasound tech will note the uterine size, shape, and position.
If the ultrasound is 3D, it may also be possible to visualize certain uterine abnormalities, like a bicornuate or septate uterus.
The technician will also look for any indication of uterine masses, like fibroids, polyps, or an adenomyosis.
These can’t always be seen with a regular ultrasound. Further evaluation may require a sonohysterogram or a hysteroscopy.
Endometrium thickness: The lining of the uterus, the endometrium, thickens and changes as your menstrual cycle progresses.
The technician will look for healthy indications that the endometrium is at the stage it should be, based on the day of your exam.
The ultrasound tech will also measure the thickness of the endometrium. It should be thin before ovulation and thicker after ovulation.
Possibly fallopian tube problems: A basic ultrasound isn’t capable of capturing healthy fallopian tubes. However, a fallopian tube may be seen with a regular 2D ultrasound if it is swollen or filled with fluid, which can occur with a hydrosalpinx.
A basic ultrasound can’t determine if the fallopian tubes are clear and open. To evaluate whether the tubes are open or closed, your doctor will most likely order an HSG.
However, with a specialized ultrasound known as a hysterosalpingo-contrast sonography (HyCoSy), your doctor may be able to detect whether the tubes are blocked or not.
Possible evidence of adhesions: By gently pressing on the reproductive organs with the transvaginal transducer, the technician can see if the organs move freely and as they should, or if they seem to adhere to each other.
The tech may also use the ultrasound wand to gentle push at the ovaries, to see how they move around in the pelvic cavity. Ovaries that seem stuck to each other are sometimes called “kissing ovaries.”
Adhesions may prevent the reproductive organs from freely moving. Adhesions can form from a previous pelvic infection or from endometriosis.
Blood flow to reproductive organs: if your doctor is using colour Doppler, the technician may be able to evaluate blood flow around a cyst or mass. This can help distinguish between a healthy cyst, an endometrial cyst (endometrioma), or an ovarian tumor.
What Can’t an Ultrasound Evaluate?
Ultrasound can’t diagnose or rule out the following:
Blocked fallopian tubes: With the exception of a hysterosalpingo-contrast sonography (HyCoSy), a basic ultrasound can’t evaluate the fallopian tubes.
Endometriosis: Only laparoscopic surgery can diagnose endometriosis.
While it’s possible to sometime see indications of severe endometriosis on an ultrasound, moderate and less severe cases are not typically visible.
Some uterine abnormalities: a general ultrasound is unlikely to catch or diagnose certain uterine abnormalities.
A sonohysterogram may be required, or the more invasive hysteroscopy, to fully evaluate the uterus.
Ultrasound Scans During Fertility Treatment
Ultrasound scans are an important part of fertility treatment monitoring.
Ultrasound isn’t usually used to monitor Clomid cycles if you’re seeing a regular OB/GYN, but it may be used if you are going to a fertility clinic.
Ultrasound is frequently used to monitor gonadotropin cycles and always used during IVF treatment cycles.
Here is what to expect.
Baseline ultrasound scan: Your doctor will likely tell you to call their office on the first day of your period, the month of your scheduled treatment cycle. They will want to schedule blood work and an ultrasound within the next few days.
This is known as your baseline ultrasound. The purpose is to check that there are no unusual cysts on the ovaries before starting the fertility drugs.
Sometimes, a stubborn corpus luteum cyst sticks around even after your period starts. This isn’t dangerous and will usually go away without intervention. However, treatment may be delayed in the meantime. Fertility drugs could exasperate the cyst.
(This first transvaginal ultrasound will likely occur when you are menstruating. While this can be an uncomfortable experience, it is nothing to be embarrassed about. You are not the first woman to be on her period during an ultrasound exam. This doesn’t bother the ultrasound technician at all.)
Follicle growth: This is the number one monitoring focus during fertility treatment. These are all transvaginal ultrasound scans, and, depending on your treatment, you may be at the clinic every couple of days for one of these scans.
The doctor or ultrasound tech will be looking to see how many follicles are developing and how quickly they are growing. Your fertility medications may be adjusted up or down, depending on follicle growth.
Once the follicles reach a particular size, your “trigger shot” (an injection of hCG) or the egg retrieval will be scheduled.
It is also possible that too few or too many follicles may develop.
If you are going through IVF treatment, and few to no follicles are appearing, your cycle may be cancelled.
If you are having IUI or gonadotropin treatment, and too many follicles are growing, your cycle may be cancelled to avoid the risk of having a high-order multiple pregnancy.
Endometrial thickness: The ultrasound tech will also likely measure your endometrial thickness. Based on this information, your doctor may change your fertility medication dosages.
Ultrasound-guided procedures: Not a part of monitoring, ultrasound may also be used during treatment itself.
During egg retrieval, for IVF treatment, an ultrasound-guided needle is used to retrieve eggs from the ovaries. Some doctors also use ultrasound during embryo transfer.
Ultrasound Scan in Very Early Pregnancy
If you get pregnant during fertility treatment, you won’t be sent right away back to your regular OB/GYN. Your fertility doctor will first want to be sure the pregnancy is progressing as expected, at least in the early weeks.
The first ultrasound will likely be scheduled around week six. This is two weeks past your expected period or pregnancy test day. The technician will be looking for a gestational sac. It is very unlikely a heartbeat will be detected at this point, so don’t get upset if you don’t see one.
Your doctor will also be looking to see if you are carrying multiples. At this stage, it is not always possible to see for certain if you are carrying more than one.
Once a gestational sac has been visualized, the pregnancy is considered to be a clinical pregnancy. (A chemical pregnancy is when blood work detects pregnancy hormone, but there are not yet any other visible pregnancy signs.)
A couple weeks later, you will likely have another ultrasound. This will be to look for a fetal pole and hopefully a heartbeat. They will also again try to verify whether you are carrying a singleton, twins, or more.
Once a heartbeat is detected, you’ll be sent to your regular OB/GYN for prenatal care. Even after infertility, a high-risk OB/GYN isn’t usually needed in a healthy pregnancy.